
1008
PROSPECTIVE RANDOMIZED COMPARISON OF PRECUT PAPILLOTOMY(PCP) AND ENDOSONOGRAPHY GUIDED RENDEZVOUS(EUSRV)PROCEDURE FOR BILE DUCT ACCESS IN PATIENTS WITH DISTAL CBD OBSTRUCTION AND DIFFICULT CBD CANNULATION
Date
May 21, 2024
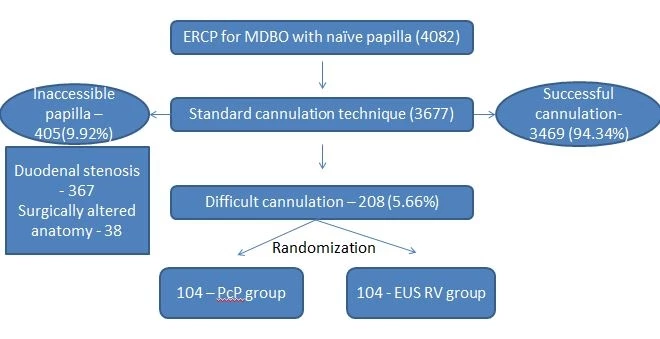
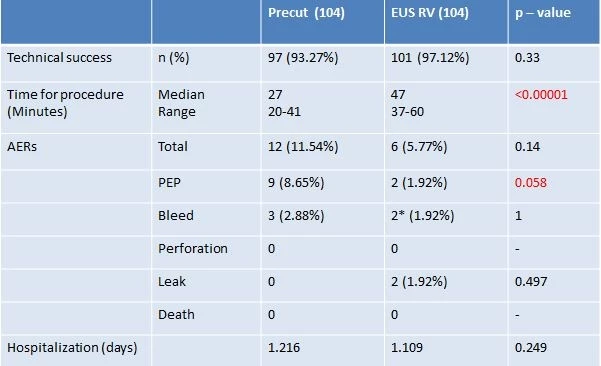
Introduction: Difficult biliary cannulation needs additional endoscopic procedures to achieve selective biliary access, with possibility of increased adverse event rate (AER) like pancreatitis. We previously showed that EUS-RV had a higher single session success rate than precut papillotomy in these patients, in a retrospective study. The present randomized study aims at comparing the technical success and AER. between the two approaches. Methods: This was an open label randomized controlled trial. We enrolled patients with initial failed attempt at cannulation defined by 5 or more attempts with the guidewire or exceeding more than 5mins. Patients with inaccessible papilla (duodenal stenosis / surgically altered anatomy), previous sphincterotomy and patients with bleeding tendencies were excluded. In the PcP group standard precut sphincterotomy was performed using needle knife sphincterotome while in the EUSRV group, initial attempt was made from the duodenal bulb using 19G FNA needle and passing the guidewire across the stricture into the duodenum, followed by scope exchange and CBD cannulation alongside the previously placed guidewire. In cases with large lesions and multiple collaterals intrahepatic route was opted for initial puncture. The primary outcome was technical success, while secondary outcomes were AER, procedure duration, and hospital stay . Randomization was done using random number generator. Continuous variables were compared using unpaired t test. Categorical variables were compared using the Chi square test/Fishers exact test as indicated. Statistical significance was determined at p < 0.05 Results: A total of 208 patients were enrolled, 104 in each group (123 males, 59.13%). All baseline demographics data were comparable between the two groups . There was no significant difference in terms of technical success (93.27% PcP vs 97.12% EUSRV, p =0.33), overall AER (11.54% PcP vs 5.77% EUSRV, p =0.14) or mortality (Zero in either group). Pancreatitis was higher in the PcP group (8.65% vs 1.92%, p = 0.058). Mean duration of procedure was significantly higher for EUSRV (47.15mins vs 27.17 min.,p <0.00001). Duration of hospitalization was similar in the two groups (1.216 PcP vs 1.109 days EUSRV, p =0.249). Conclusion: Both PcP and EUSRV have comparable success, AER, mortality, and hospitalization. PcP has higher rates of pancreatitis while EUSRV needs longer procedure time. EUSRV is a viable alternative to PcP in centres with expertise.(CTRI/2012/12/003248 [Registered on: 20/12/2012])
Patient accrual
Results
Presenter

Institute of Digestive and Liver Care, SL Raheja Hospital
Tracks
Related Products

EUS-GUIDED BALLOON OCCLUDED GASTROJEJUNOSTOMY BYPASS (EPASS) VERSUS DUODENAL STENT FOR UNRESECTABLE MALIGNANT GASTRIC OUTLET OBSTRUCTION (DRA-GOO)
EUS-guided gastroenterostomy (EUS-GE) is a novel method for palliating gastric outlet obstructon due to unresectable malignancies…
