
128
FEASIBILITY AND CLINICAL UTILITY OF STONE EXTRACTION BALLOON CATHETER-ASSISTED ENDOSCOPIC STENTING FOR MALIGNANT DISTAL DUODENAL AND PROXIMAL JEJUNAL OBSTRUCTION
Date
May 18, 2024
Background: Endoscopic stenting for malignant distal duodenal and jejunal obstructions is challenging because the length of conventional gastroscopes is insufficient to reach the obstruction point. A stone extraction balloon catheter fully inflated after being introduced through the endoscope’s working channel can freely navigate the duodenum and jejunum without causing bowel injury by burying the catheter tip. It can easily change its direction for guidewire relocation, conforming to angulation of the small bowel flexure. This study evaluated the feasibility and efficacy of stone extraction balloon catheter-assisted endoscopic stenting for malignant distal duodenal and proximal jejunal obstructions.
Methods: Patients with malignant distal duodenal or jejunal obstruction who underwent stone extraction balloon catheter-assisted distal duodenal and proximal jejunal stenting between January 2015 and December 2022 were retrospectively analyzed.
Results: We enrolled 30 patients in this study. Pancreatic cancer was the primary cause of duodenal obstruction, with the third portion of the duodenum being the most common site of obstruction. Technical success was achieved in 100%, and the clinical success rate was 100%. The median procedure time was 35 minutes, and the mean gastric outlet obstruction score (GOOSS) improved from 1.20 (pre-procedure) to 2.87 (post-procedure). Early stent migration was encountered in one patient. During follow-up, stent dysfunction was noted in nine (30%) patients, and overall stent patency time was 145 days.
Conclusions: Stone extraction balloon catheter-assisted endoscopic stenting is an effective and reproducible technique for treating malignant distal duodenal and jejunal obstructions.
Methods: Patients with malignant distal duodenal or jejunal obstruction who underwent stone extraction balloon catheter-assisted distal duodenal and proximal jejunal stenting between January 2015 and December 2022 were retrospectively analyzed.
Results: We enrolled 30 patients in this study. Pancreatic cancer was the primary cause of duodenal obstruction, with the third portion of the duodenum being the most common site of obstruction. Technical success was achieved in 100%, and the clinical success rate was 100%. The median procedure time was 35 minutes, and the mean gastric outlet obstruction score (GOOSS) improved from 1.20 (pre-procedure) to 2.87 (post-procedure). Early stent migration was encountered in one patient. During follow-up, stent dysfunction was noted in nine (30%) patients, and overall stent patency time was 145 days.
Conclusions: Stone extraction balloon catheter-assisted endoscopic stenting is an effective and reproducible technique for treating malignant distal duodenal and jejunal obstructions.
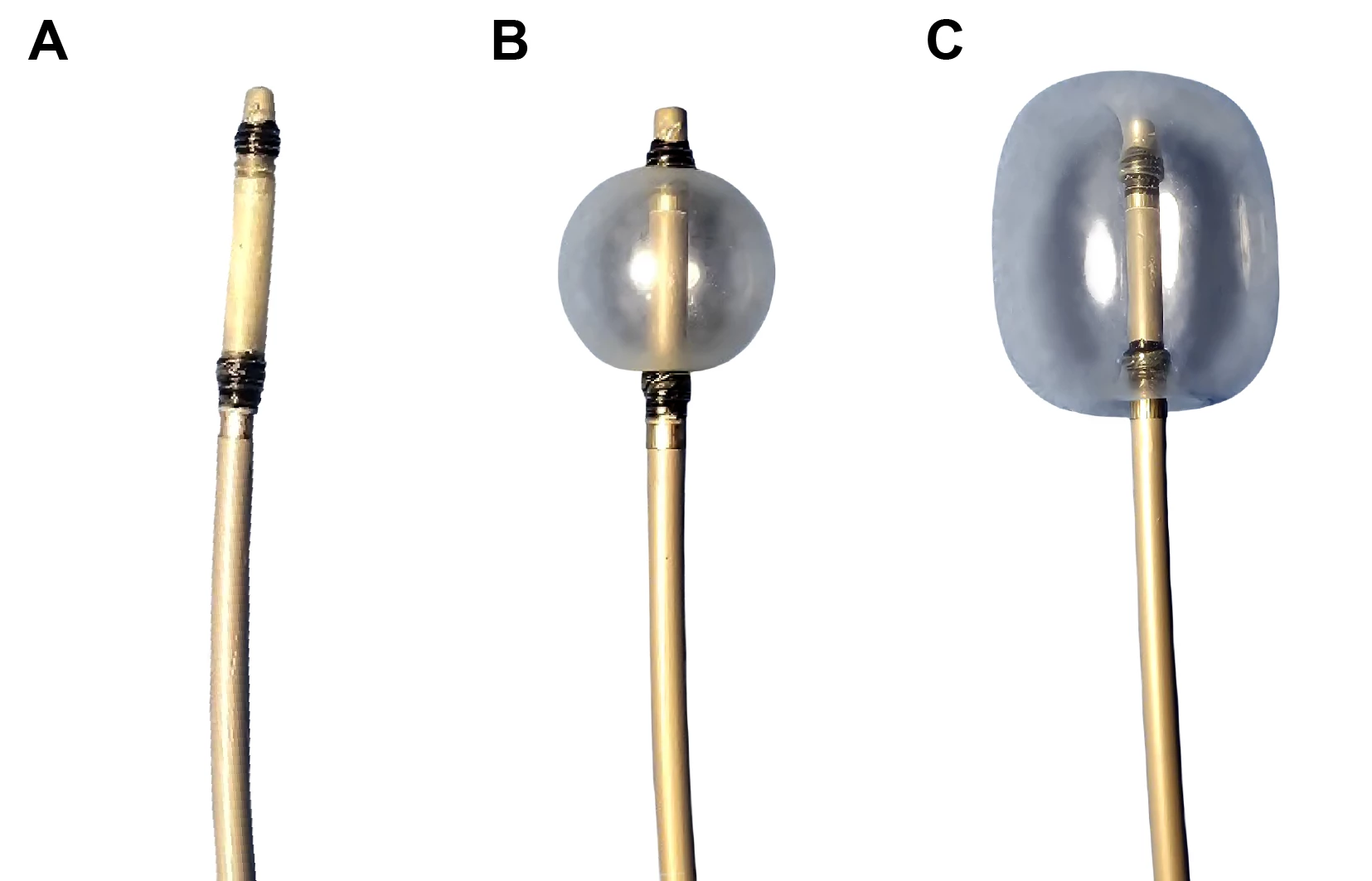
The tip of the triple-lumen balloon catheter is buried by the fully inflated balloon.
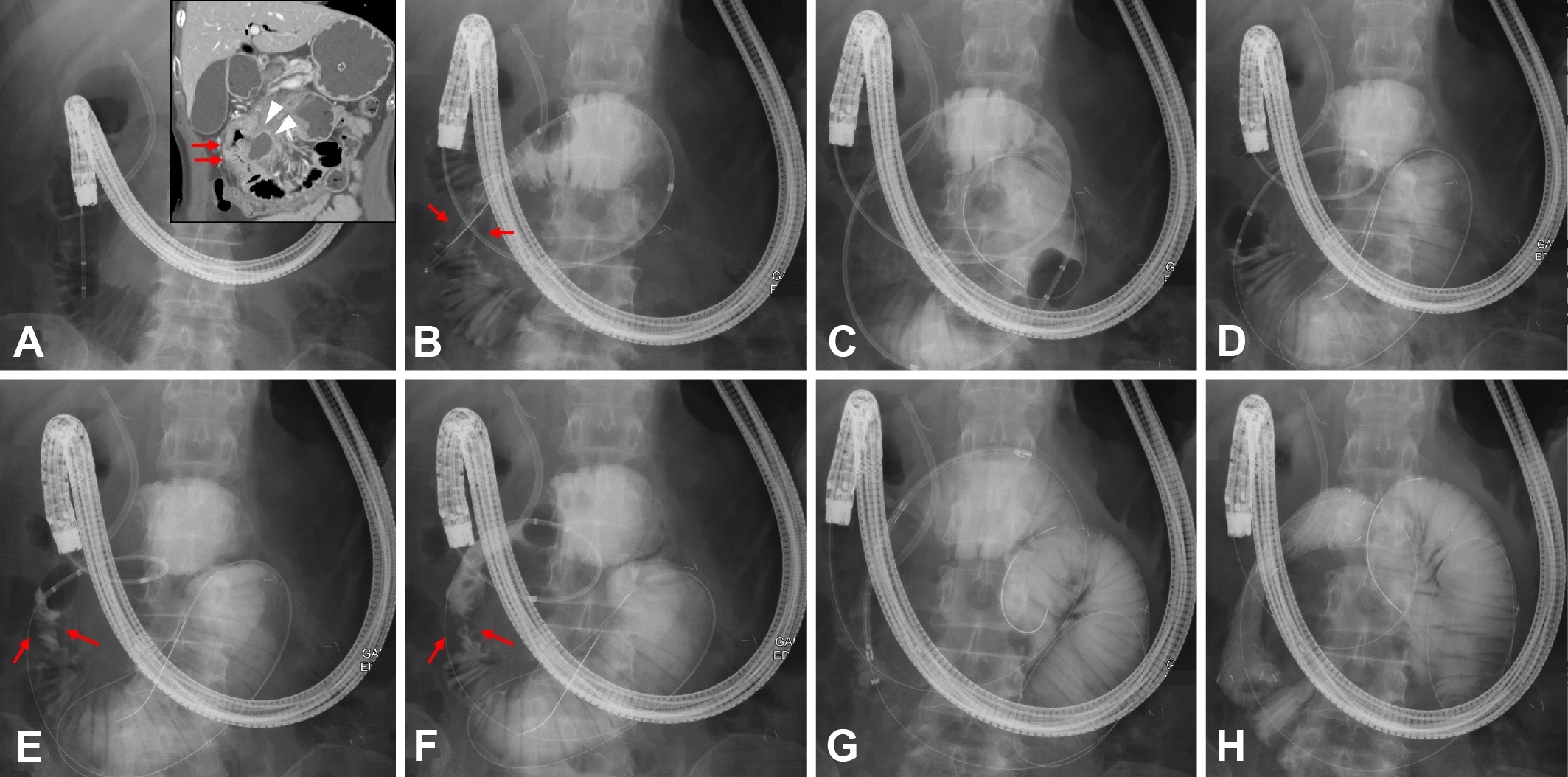
Stone extraction balloon catheter-assisted endoscopic stenting for malignant proximal jejunal obstruction caused by a malignant mesenteric lymph node (red arrows: jejunal obstruction; white arrowheads: mesenteric lymph node).
Presenter
Speaker

Johns Hopkins
Tracks
Related Products

“MYSELF” - A NOVEL AND EASY-TO-IMPLEMENT PRE-PROCEDURE ERGONOMIC TIME-OUT THAT REDUCES ENDOSCOPISTS’ RISK OF MUSCULOSKELETAL INJURY
BACKGROUND: Implementing ergonomic principles in the endoscopy unit can mitigate the risk of endoscopy related injury. An efficient and effective training tool is needed to facilitate ergonomic endoscopy…
DEVELOPMENT OF AMERICAN SOCIETY FOR GASTROINTESTINAL ENDOSCOPY (ASGE) MINIMUM STANDARDS FOR TRAINING IN INTERVENTIONAL ENDOSCOPY WITHIN DEDICATED INTERVENTIONAL ENDOSCOPY FELLOWSHIP PROGRAMS
BACKGROUND: There is a lack of data on training benchmarks to define competence in colorectal EMR (C-EMR) among advanced endoscopy trainees (AETs). Previous pilot data from our group demonstrated a relatively low proportion of AETs achieve competence on key cognitive and technical aspects of C-EMR…
