
923
AN EDGI FIX FOR A RARE CAUSE OF GI BLEEDING: EUS-GLUE/COIL OF A BLEEDING DUODENAL VARIX VIA EUS-DIRECTED TRANSGASTRIC INTERVENTION
Date
May 20, 2024
Introduction: Duodenal varices are rare causes of bleeding, which can be treated with EUS visualization and injection of glue with coil embolization. EUS-directed transgastric intervention (EDGI) is a novel approach for patients with prior Roux-en-Y gastric bypass (RYGB) and pathology in the biliopancreatic limb. We present a case of successful EDGI and EUS-glue/coil ablation of a bleeding duodenal varix in a patient with prior RYGB.
Case: A 43-year-old woman with a history of RYGB presented with melena and was found to have a hemoglobin of 6.9 g/dL due to bleeding esophageal varices (EV). Her RYGB history was complicated by superior mesenteric and portal vein thromboses, leading to non-cirrhotic portal hypertension with prior EV and gastric varices, previously treated with band ligation, glue/coil, and TIPS. Despite EV banding on admission, she continued to have melena and transfusion-refractory anemia. Second look EGD and colonoscopy revealed no other culprit lesion. Upon transfer to our facility, a rigidizing overtube-assisted enteroscopy up the biliopancreatic limb revealed an intermittently bleeding varix in the third portion of the duodenum. The linear echoendoscope with the rigidized overtube was too short to reach the culprit lesion. Due to limited interventional radiology and surgical options, multidisciplinary discussions determined that EDGI with EUS-glue/coil would be the best management option.
For the EDGI, a 19-gauge FNA needle was advanced across the gastric pouch into the excluded stomach under EUS guidance and confirmed with contrast injection under fluoroscopy. The stomach was filled with 500 mL of sterile water and contrast. Under EUS, a 20 mm lumen apposing metal stent (LAMS) was used to create a gastrogastrostomy between the gastric pouch and excluded stomach. Due to the angulation of the stomach, the LAMS was sutured in place (Figure 1) and EUS-glue/coil was delayed for tract maturation to minimize LAMS migration. After one week, the linear echoendoscope was successfully advanced through the gastrogastrostomy to the duodenum and the 9 mm duodenal varix was treated with embolization coils (three 15 mm and one 12 mm) and 1.5 mL of cyanoacrylate with complete varix ablation (Figure 2).
EUS two months later showed a resolved duodenal varix. The LAMS was removed, and the fistula sutured closed.
Discussion: Duodenal varices are rare, and EUS-glue/coil offers a successful treatment option. For those with prior RYGB, EDGI is a novel technique that allows for anterograde access to the excluded stomach and biliopancreatic limb for intervention. Previously documented EDGI uses have mostly been for diagnostic EUS of extraluminal pathology. To date, this is the first documented successful EDGI with EUS-glue/coil for a duodenal varix. This highlights the feasibility of EDGI and range of therapeutic interventions possible.
Case: A 43-year-old woman with a history of RYGB presented with melena and was found to have a hemoglobin of 6.9 g/dL due to bleeding esophageal varices (EV). Her RYGB history was complicated by superior mesenteric and portal vein thromboses, leading to non-cirrhotic portal hypertension with prior EV and gastric varices, previously treated with band ligation, glue/coil, and TIPS. Despite EV banding on admission, she continued to have melena and transfusion-refractory anemia. Second look EGD and colonoscopy revealed no other culprit lesion. Upon transfer to our facility, a rigidizing overtube-assisted enteroscopy up the biliopancreatic limb revealed an intermittently bleeding varix in the third portion of the duodenum. The linear echoendoscope with the rigidized overtube was too short to reach the culprit lesion. Due to limited interventional radiology and surgical options, multidisciplinary discussions determined that EDGI with EUS-glue/coil would be the best management option.
For the EDGI, a 19-gauge FNA needle was advanced across the gastric pouch into the excluded stomach under EUS guidance and confirmed with contrast injection under fluoroscopy. The stomach was filled with 500 mL of sterile water and contrast. Under EUS, a 20 mm lumen apposing metal stent (LAMS) was used to create a gastrogastrostomy between the gastric pouch and excluded stomach. Due to the angulation of the stomach, the LAMS was sutured in place (Figure 1) and EUS-glue/coil was delayed for tract maturation to minimize LAMS migration. After one week, the linear echoendoscope was successfully advanced through the gastrogastrostomy to the duodenum and the 9 mm duodenal varix was treated with embolization coils (three 15 mm and one 12 mm) and 1.5 mL of cyanoacrylate with complete varix ablation (Figure 2).
EUS two months later showed a resolved duodenal varix. The LAMS was removed, and the fistula sutured closed.
Discussion: Duodenal varices are rare, and EUS-glue/coil offers a successful treatment option. For those with prior RYGB, EDGI is a novel technique that allows for anterograde access to the excluded stomach and biliopancreatic limb for intervention. Previously documented EDGI uses have mostly been for diagnostic EUS of extraluminal pathology. To date, this is the first documented successful EDGI with EUS-glue/coil for a duodenal varix. This highlights the feasibility of EDGI and range of therapeutic interventions possible.
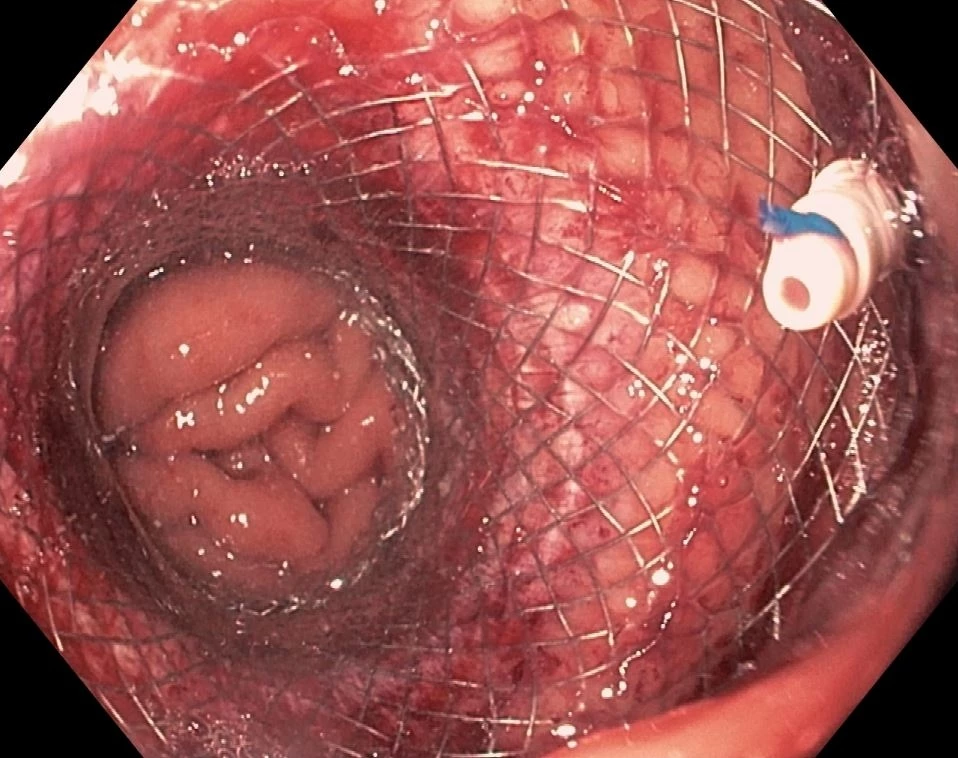
Figure 1. EDGI Gastrogastrostomy with Sutured LAMS
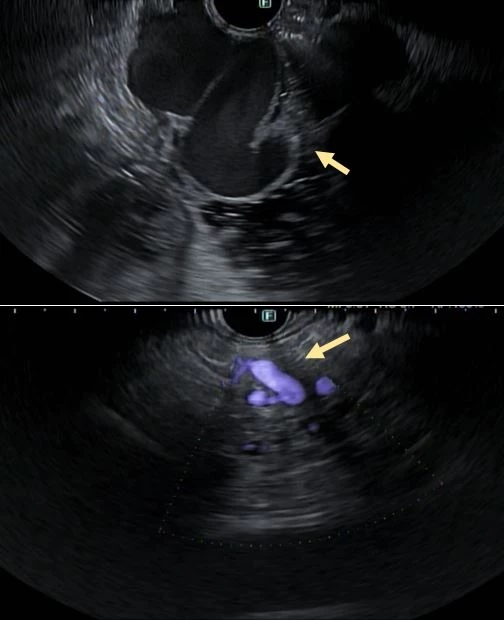
Figure 2. Duodenal Varix Pre- (Top) And Post- (Bottom) EUS-glue/coil Ablation
Presenter

Speakers
Tracks
Related Products

INTRODUCTIONS
SOCIETY: ASGE
COMPARISON OF ENTEROSCOPY-ASSISTED ERCP VERSUS EUS-GUIDED BILIARY INTERVENTION VERSUS EUS-DIRECTED TRANSGASTRIC ERCP IN PATIENTS WITH ROUX-EN-Y GASTRIC BYPASS.
Ampullary neoplasia (AN) is a rare disease, but its incidence is increasing…
